


US Health Insurance Basics
Alright, this post is about the very high-level stuff a health tech person should know about health insurance in the US. As always, tried to keep the content short but helpful and link out liberally if you want to go deeper.
Here’s a button in case you want to get my next post in your inbox:
Players
This is an overview of the terms for the people and institutions involved in health insurance payment.
Payers
This usually refers to institutions (not individuals) that pay for medical services for the most part this means health insurance companies, government insurance, or employers that pay directly for some healthcare services.
Members
The person who signs up to a payer’s plan. Usually but not always the beneficiary.
Beneficiary
The person who benefits from the service that is being paid for. Often it is the member or a dependent of the member.
Providers
Health care clinician who provides a service to a person. This could be a doctor, nurse, physician’s assistant, therapist or other.
Network
The group of providers who can give care to patients and receive payments from a specific payers. For example, my HMO plan only allows me to go to certain providers and those providers constitute a ‘network’
Payments
This is a very brief guide to payment terms and concepts, like co-pays, co-insurance, etc. etc.
This is a pretty good graphic from the CMS:

(from this: https://www.cms.gov/CCIIO/Resources/Forms-Reports-and-Other-Resources/Downloads/uniform-glossary-final.pdf)
Monthly premium
A monthly payment on behalf of member to be covered by a payer plan. This is often partly or fully covered by an employer, but can be fully or partly paid by an individual as well.
eg. My employer pays $XX/ month so I can have health insurance coveraged. Because I have a plan with greater coverage, I pay an additional $XX / month. These are premiums.
Yearly deductible
The amount that has to be paid out-of-pocket by a member before the payer starts contributing to health care payments.
Co-pay
An amount that a member has to pay for each health care visit or services, even if the rest is covered by the payer
Co-insurance
When a bill is split between a member’s out-of-pocket cost and a payment from the payer.
Out-of-pocket Maximum
When Jane pays a certain amount of money for health care coverage, either in co-pay, co-insurance or deductibles, over the course of the year, a payer often will cover everything after that. That amount of money is called the ‘out-of-pocket maximum’
Major Payer Types
Here we’re going to give some info about some of the major payers in the ecosystem and what the plans and coverage might look like.
For an idea of the scale and proportions of this ecosystem this is a good graphic from Which Country Has the World’s Best Healthcare by Ezekial Emanuel. Numbers are from 2017 and may or may not match numbers later in this section.

(from Which Country Has the World’s Best Healthcare by Ezekial Emanuel)
AND THIS graphic does a good job of explaining who is covered by which insurance programs. I saw it in a Coursera MOOC on value based care, linked in the caption.
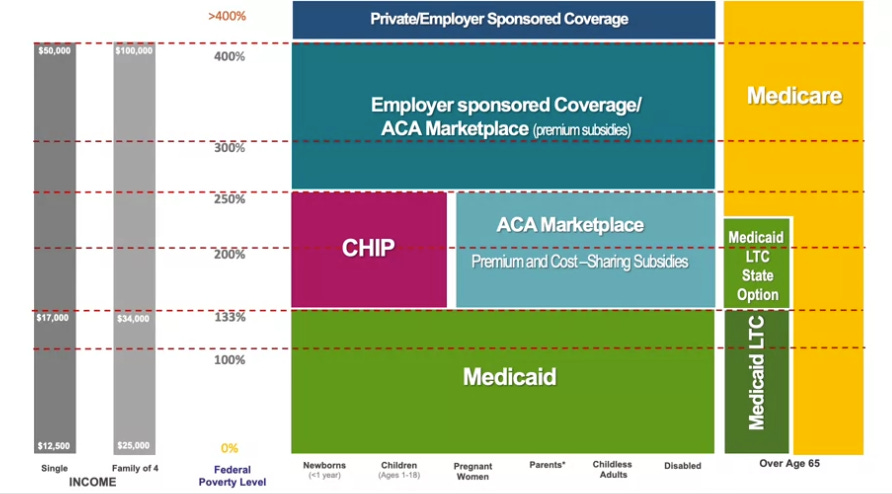
Now I’ll do a quick step through of the major payers from those graphics.
Commercial Insurance
Commercial Insurance provides coverage to ~150-180 million people.
It can either be paid by the individual or by a sponsoring employer.
In 2017, Employer sponsored commercial insurance covered about half of all Americans.
I hope to do some more writing on the biggest commercial payers but I’m just going to leave that out of scope for now.
Instead, I’m going to give a brief outline of the major types of plans.
HMO - Health Maintenance Organization
HMOs are generally cheaper plans that became popular in the 1990s. Visits are only covered if the member visits a doctor in the HMO network.
They may require patients to select a PCP (Primary Care Physician) and get that PCP to refer the member if they require specialty care.
HMOs tend to have low premiums and low or no deductibles.
PPO - Preferred Provider Organization
PPOs are a type of commercial managed care plan with more flexibility than HMOs. There is still a provider network with generally lower rates, but there are fewer restrictions about seeing non-network providers.
Generally, members can see specialists without a PCP referral and can go to out-of-network doctors or hospitals at higher out-of-pocket costs.
POS - Point of service
POS plans are kind of like a hybrid of PPO and HMO plans.
Similar to HMOs, members of a POS choose an in-network PCP, but like a PPO they can go out of network for services if they wish.
ACA plans - Affordable Care Act
The Affordable Care Act, passed during the Obama administration in 2010, expanded Medicaid, and established online exchanges for individuals to purchase health insurance. It also funded subsidies for certain low-income individuals.
The ACA forbids plans purchased on the exchanges from excluding coverage for pre-existing conditions.
Individual plans accounted for 15 Million lives in 2017, 11 Million of which were purchased in ACA exchanges.
Government Programs
Medicare and Medicaid founded in the Social Security Amendments of 1965 to pay for medical care for those who did not have or could not afford private health insurance.
It now consists of two large programs, Medicare & Medicaid, and smaller programs for the Military, Veterans and Indian Health Service.
This graphic does a pretty good job of outlining the differences and overlaps between Medicare & Medicaid. It’s from the same Coursera MOOC linked above.
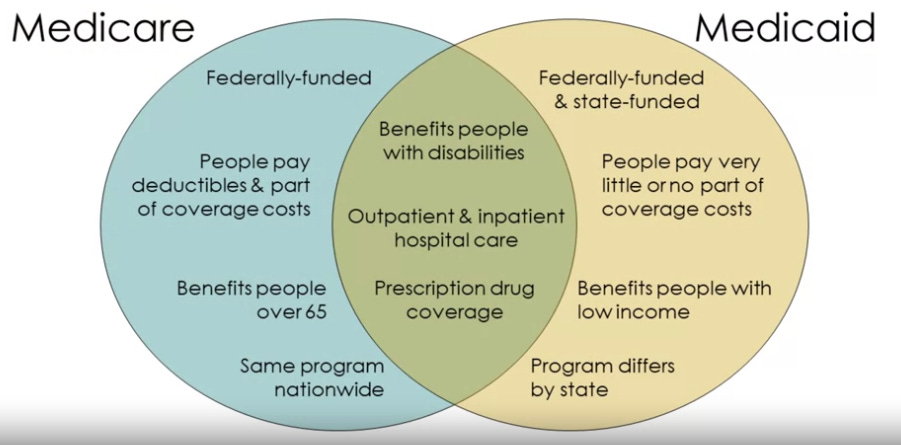
(from https://www.coursera.org/learn/value-based-care-introduction/home/week/2)
Medicare
Medicare is a health insurance program run by the federal government. It pays for health care services for about 60 million people (2018), primarily those aged 65+ as well as people with some disabilities and patients with end-stage renal disease.
Members pay small monthly premiums for non-hospital coverage, which differ based on income levels.
Medicare programs are divided into four parts.
Part A - Covers inpatient hospital, skilled nursing facility care, hospice, home health care
Part B - Helps cover routine doctors visits, preventative care, mental health care, supplies. Patients can also buy Medicare Supplement Insurance plan to help pay.
Part C - This part includes Medicare Advantage (MA) plans. MA plans are Medicare plans offered through private insurance companies. They can include dental, vision and other services not covered through original medicare. Added in 1997. Continues to grow as a proportion of Medicare participants(see graph below)
Part D - Covers prescription drugs. Funded by the federal government and administered through private insurance companies. It’s a relatively new program, founded in 2006.

Medicaid
Medicaid is a more complex program. It covers 71 million people as of 2020, including those covered by CHIP (Childrens Health Insurance Program, explained below). Medicaid accounts for about a a fifth of total healthcare spending in the US.
States and territories administer Medicaid with Federal funding. The programs serve low income patients of any age. Small co-pay sometimes required but co-pays and coverage varies by state.
Medicaid programs are ‘means tested’, which means that beneficiaries income and savings are taken into account when determining coverage.
States have flexibility to determine who is covered and how payments work, but the minimum income level for coverage is 133% of the federal poverty line. Many states cover higher income levels than that, though. All this means considerable differences in spending and coverage by state.
Nearly half of all US children are covered by medicaid or a similar program (like CHIP) and Medicaid is the largest payor of nursing home care in US.
CHIP - Children’s Health Insurance Program
CHIP is a program enacted in the 1990s that provides coverage for children whose families have incomes too high to qualify them for Medicaid but still struggle to afford private insurance.
CHIP is administered by the states and work closely with the Medicaid programs
BHP - Basic Health Program
BHP is another program affiliated with Medicaid and designed for people whose income fluctuates above and below the Medicaid cut off.
It was introduced as part of the Affordable Care Act.
TRICARE -
TRICARE can be thought of as employer-sponsored insurance for active-duty service members, National Guard and Reserve members, retirees, and their family members and survivors. It covers about 9.4 million people as of 2020. Because the employer is the US government, it is also a government-sponsored program.
There are 11 different plans administered by commercial insurance companies and out of pocket varies depending on whether care received in military facilities.
VHA - Veterans Health Administration
The VHA is administered by the Department of Veteran’s Affairs (the VA). The VHA runs 1200 medical facilities, medical centers, out-patient clinics, community-based clinics and long-term facilities, as well as providing payment for certain veterans.
In order to be eligible for coverage by the VHA, a person must be a veteran with over 180 days of military service, received an honorable discharge and have a service related illness, injury, disability or live in poverty.
80% of those covered by the VHA have additional health insurance coverage.
Resources
In addition to the links I provided in the body, these are some good reads:
https://www.healthsystemtracker.org/
https://www.kff.org/medicare/video/medicare-and-medicaid-at-50/
https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/
https://www.healthcare.gov/glossary/